
FDA Should Rescind EUA Approvals for All COVID-19 Rapid Antigen Test Methods
Greatly Reduced Sensitivity With Variants Translates to Unacceptable False Negative Rates and a Worsening of the Pandemic


Full disclosure. I currently work in research and development for a company which develops and sells both rapid antigen and RT-qPCR test kits and provides testing services for Covid-19. Hopefully it goes without saying that the opinions expressed here are my own and not necessarily endorsed nor shared by my employer.
Background
We have known since basically day one that the various rapid antigen test kits (lateral flow based tests) on the market were not as sensitive as RT-qPCR (the gold standard laboratory based method) for the detection of SARS-CoV-2. We accepted this performance difference as a necessary evil because rapid antigen methods have many advantages over RT-qPCR when it comes to usefulness in diagnosing SARS-CoV-2 infections in large numbers of people. Chief among them are cost and the ability to be run directly at a doctors office or in the home. Because they are so inexpensive and easy to use they can be used to screen huge numbers of people at very little cost and without the need for highly skilled technicians or specialized laboratories to run the tests.
The paper and the data
A new paper in Nature Scientific Reports raises alarm bells about the potential usefulness (or not) of these rapid antigen screening methods. It illustrates in great detail just how badly these tests perform compared to RT-PCR especially with the newer SARS-CoV-2 variants, and even more so, when used by consumers to test themselves in their own homes. In my opinion, the data is so bad that it justifies the immediate suspension of all EUA approvals so far granted to the various rapid antigen methods currently on the market. I will get to the why shortly but first let's have a look at the data.
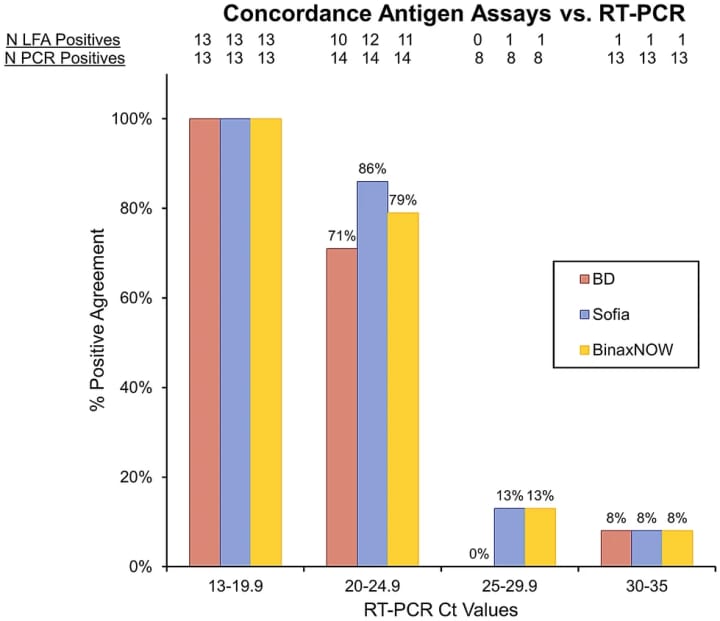
Figure 1 from the paper which I am showing above is about as damning as it gets and tells you everything you need to know in one handy little bar graph. For those who are not qPCR experts let me try and explain it simply and at a very high level. The lower the Ct value (values on the X-axis) the higher the concentration of virus. (note: Because of the exponential nature of PCR amplification and a fascinating feature of math every 3.3Ct's equals a one log concentration change. So a Ct of ~16 would be~1 log more concentrated than a sample with a Ct ~19. I realize most people are not used to dealing with log values on a regular basis. Linked here is something I wrote a while back that might help some. In the above figure virus concentrations span a >6.5 log range, as low as 13 to as high as 35, which is pretty amazing in an of itself and says something about the large diversity in viral loads in infected persons at different times of infection and with different variants.)
Ct values in the 13-19.9 range indicate an extremely high level of virus and the fact that so many clinical samples showed these low Ct values is alarming in and of itself, however, that not notwithstanding, the key takeaway is that lower Ct equals higher input viral load into the test. At those high virus levels one would expect the rapid antigen methods to easily detect the virus just as the qPCR method does and in fact that is what you do see. 100% agreement between the rapid antigen methods and RT-qPCR. However, as Ct values trend upwards (remember that means lower concentration of virus present) we start to see rapid antigen method negatives that were easily positive by qPCR. As a qPCR expert I am frankly shocked at the fact that the rapid antigen methods are missing qPCR positives in the 20-25Ct range. Those Ct values are still indicative of very high levels of virus and I would have expected them to be easily detected as well by just about any method one could dream up. The fact that they are not is very worrisome indeed. Even Ct values of 25-30 indicate a reasonably high viral load and the fact that only 0-13% of positive PCR samples were called positive by a rapid antigen method is shocking and disturbing. These are real world clinical samples, not artificially inoculated test samples. The results of those tests are described in other parts of the paper and they tell a similar tale. Rapid antigen method sensitivity is terrible and has continued getting worse with each successive variant. This is not all that surprising given the predicted impacts of the known mutations of each of the variants but I don't think anyone predicted the sensitivity drop off to be as dramatic as it has been.
The consequences of high false negative rates
So what's the bid deal you may be asking yourself. So what if the test is less sensitive, it still detects the virus and it is better than nothing, right? Previously, I was in this camp and agreed that even a flawed test was much much better than nothing. However, things have changed significantly since those early days of the pandemic. We now have insurance companies refusing to pay for RT-qPCR testing, and/or even worse, refusing to pay Covid-19 benefits to anyone who does not have a positive test result. The cynic in me says they are actually pushing the antigen tests because they know all this. However, I am refusing to give into that cynic for the moment and continue to believe they are trying to do the right thing here. Until now they have simply not been aware of just how poorly the antigen tests actually perform. That excuse is now gone. In addition to and as a consequence of insurance companies decisions with respect to Covid-19 we also have employers refusing to allow their employees to stay home from work (and receive covid-19 benefits) without a positive test result. Even worse, you can basically forget about getting the appropriate course of treatment at an emergency room or at a hospital because without a positive test result most will not admit patients or treat for Covid-19 at all. All of this is a recipe for disaster. Sick people, who have almost certainly have Covid-19, are being forced by insurance companies to get a poorly performing test, and then when the test comes back negative, being forced to go into work and/or not working and not getting employer benefits associated with Covid-19. Moreover, many of these people are being denied admissions to hospitals and the appropriate therapeutics.
Health care workers take it on the chin again
And of course, as with many of the most unfortunate aspects of the pandemic, health care workers are once again taking a big chunk of the pain. Case in my point, my own primary care physician. During a recent visit the topic of Covid-19 rapid antigen test methods arose during conversation. I mentioned that both myself and my wife are researchers who had been working on various aspects of Covid-19 and mentioned the data from the paper I describe here, and my own views on the matter. She sat silently listened and nodded politely but the emotion in her eyes and in her demeanor was evident as I talked. They shifted from curious interest to concerned to disgust to anger in a manner of about 30 seconds. When I was done she explained to me that she had been out sick recently for ten days, very sick, and almost certainly had COVID-19, and almost certainly it was the delta variant given her symptoms and its prevalence in our region of the country. She explained that she had been unable to take advantage of her companies Covid-19 leave policies because she never had a positive test result, despite being tested by rapid antigen method on four separate occasions. She went on to describe how herself and the entire staff at the facility at which she works are screened regularly by rapid antigen method, and must show negative results, as a requirement of continuing to work. She also expressed concern that so few (none in fact) of the staff at the facility at which she worked had tested positive for COVID-19 in the recent past despite several coworkers who were obviously ill with typical symptoms. Without a positive test these sick workers continued to go in to work where they almost certainly exposed others. Without covid leave to cover their time off they simply could not afford to not go into work. In another perfect example of this dilemma a work colleague recently relayed the story of her mother who was very ill with what was almost certainly Covid-19 based on the symptomology and her exposure history, but had multiple negative test results by rapid antigen methods and was forced to return to work because of it. In the end she finally did get a PCR test but it was negative. Likely, the window of opportunity to catch the virus had been missed. Who knows how many other people she infected while back in the office.
Conclusions
I don't blame the test kit manufacturers or the doctors for this crappy situation we find ourselves in. I know that the test kit makers are doing the absolute best they can under extremely difficult circumstances. The tests they have managed to develop and deploy in an incredibly short amount of time are amazing and have no doubt saved countless lives. And nobody can call into to question the dedication of the thousands of doctors around the country and the world who are busting their humps day in and day out to keep people healthy and free from Covid-19 in any way they can. And believe it or not I do not blame the insurance companies or FDA either. They are doing the best they can to manage in very difficult circumstances as well. It is the fault of our own broken health care system which incentivizes the wrong behaviors and punishes the right ones by valuing the bottom line over the greater good. Until that changes situations like the one we find ourselves in now will happen again and again. In this case it is way too late to change the system but FDA could do a lot to get the ship righted by rescinding the current EUA approvals for all rapid antigen methods. The byproduct of this one decision would mean that all Covid-19 testing would have to be by RT-qPCR and insurance companies would be forced to foot the bill for it.
About the Creator
Everyday Junglist
Practicing mage of the natural sciences (Ph.D. micro/mol bio), Thought middle manager, Everyday Junglist, Boulderer, Cat lover, No tie shoelace user, Humorist, Argan oil aficionado. Occasional LinkedIn & Facebook user
Keep reading
More stories from Everyday Junglist and writers in Longevity and other communities.
Yes, You Are Allowed to Laugh at COVID-19
I know not everyone agrees, but I happen to think that anything can be made fun of. There is no topic or subject for which humor is totally off limits. Of course there is a time and a place, and a right way and a wrong way, but there is always a time, and there is always a way. When parody and satire are deployed during the midst of a tragedy, determining that time and figuring out that right way is one of the humorists' most difficult tasks. And it is a very important task. Humor is perhaps the most underrated and underutilized mechanisms we have as humans for coping with loss and remaining calm when fear threatens to overwhelm us. It does this in many ways, but I think mostly it is because it allows us to put things in their proper perspective and "take a step back." It illuminates tragedy in a way that causes us to think about it in a different way, a better way. Instead of sadness and fear, we smile and laugh, and we think maybe everything is not as bad as it seems, or even if it is, that it's not the end of the world. Yes, the pandemic is terrible, and it is tragic, but it will not result in the end of the world, and not even the most skeptical and worried of experts (I count myself among that group) are suggesting that outcome as possible even in the worst case scenarios. With all that serious stuff out of the way read on for my very few attempts (3 total) at COVID humor. Probably not my best efforts but cut me some slack, difficult topic. Gheesh. LOL!
By Everyday Junglist3 years ago in Longevity
Pints & Parkruns: Jubilee, Spennymoor
If MC Escher created a parkrun, it might look a bit like Jubilee. Based in a compact – but surprisingly lovely – park in the small County Durham town of Spennymoor, it twists and turns its way up repeated hills. Although basic physics says it must come down again, somehow this route never feels like it gives runners a proper descent.
By Andy Potts5 days ago in Longevity
Tresses in Transition: Navigating Postpartum Hair Loss with Care and Confidence
Abstract: “In the quiet moments between midnight feedings and diaper changes, I found myself staring at the mirror, bewildered by the handfuls of hair that clung to my brush. Motherhood had gifted me with boundless love, but it also bestowed upon me a less enchanting surprise: postpartum hair loss. As I embarked on this unexpected journey, I sought solace in the gentle embrace of the best shampoo for nurturing my fragile locks. Join me as we explore the science behind hair loss, the quest for the perfect shampoo, and an illuminating secret that promises to reignite our crowning glory.”
By health_kkkkeep3 days ago in Longevity



Comments
There are no comments for this story
Be the first to respond and start the conversation.