
Borderline Personality Disorder and Me
Living with BPD as a Social Worker

Borderline Personality Disorder (BPD) is often categorized — in short — as a mental illness where the survivor exhibits explosive anger, impulsive behaviors, and unstable relationships — with romantic partners, as well as friends and family. Due to the destructive nature of these symptoms, BPD has almost become a bad word in the mental health community. As an MSW, I have come across professionals who won’t work with individuals who have been diagnosed with BPD due to the stereotypical “abusive” nature of the disease. However, the symptoms listed above provide an overgeneralized assumption of the disorder based on only three out of nine possible symptoms — and all symptoms are frequently linked to trauma. This overgeneralization of BPD marginalizes survivors of the illness by belittling or oversimplifying their experience — particularly those who don’t fall under the assumed criteria. Furthermore, it makes finding help extremely difficult, let alone receiving an appropriate diagnosis. There are four types of Borderline Personality Disorder that all exhibit differently, and to be diagnosed with BPD, one must exhibit five out of nine possible criteria. The variation of symptoms then puts the survivor on a sliding scale of 256 possible representations of the disorder. Because of this, no one person fits 100% into any one of the four categories of BPD due to the number of possible variations. Survivors often exhibit symptoms that put them in more than one category — and sometimes all four — but the categories help survivors, loved ones, and professionals better understand Borderline Personality Disorder, possible causes, and treatment options.
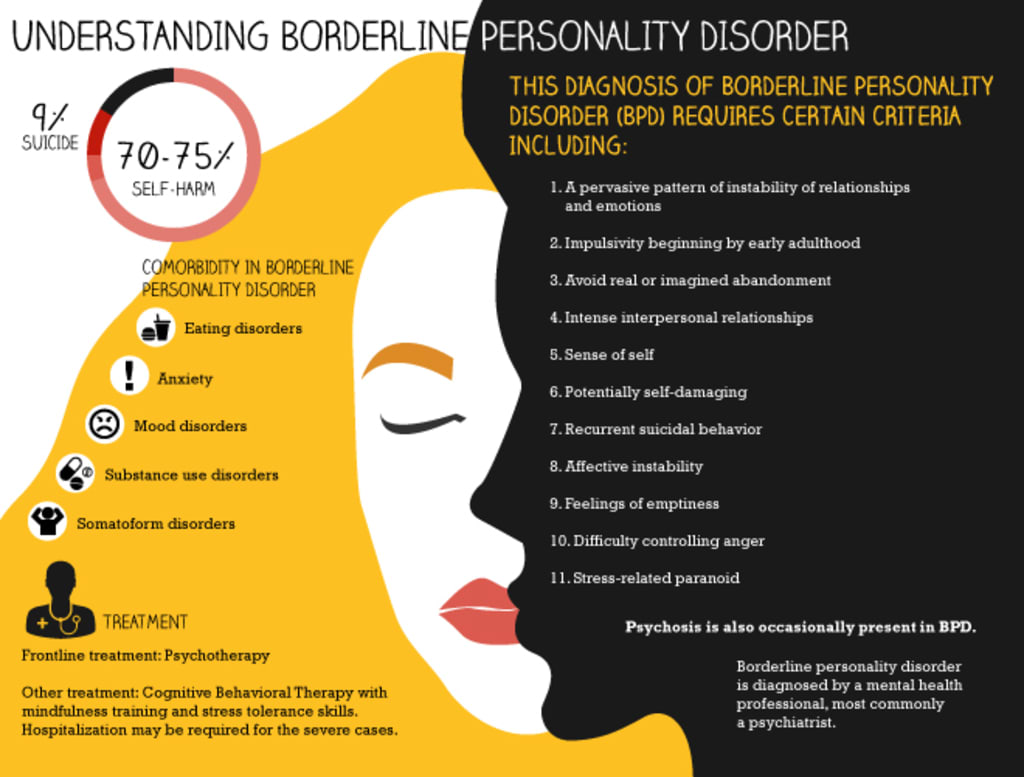
The 9 Criteria of Borderline Personality Disorder
Frantic efforts to avoid real or imagined abandonment
A pattern of unstable and intense interpersonal relationships characterized by extremes between idealization and devaluation (also known as “splitting”)
Identity disturbance: Markedly or persistently unstable self-image or sense of self
Impulsive behavior in at least two areas that are potentially self-damaging (e.g., spending, sex, substance abuse, reckless driving, binge eating)
Recurrent suicidal behavior, gestures, or threats, or self-harming behavior
Emotional instability in reaction to day-to-day events (e.g., intense episodic sadness, irritability, or anxiety usually lasting a few hours and only rarely more than a few days)
Chronic feelings of emptiness
Inappropriate, intense anger or difficulty controlling anger (e.g., frequent displays of temper, constant anger, recurrent physical fights)
Transient, stress-related paranoid ideation or severe dissociative symptoms
(Taken from the Diagnostic and Statistical Manual of Mental Disorders: Fifth Edition, 2013)
The 4 Types of Borderline Personality Disorder
Discouraged (or Quiet) BPD
Impulsive BPD
Petulant BPD
Self-Destructive BPD
My Story
I was recently diagnosed with Discouraged (or Quiet) and Petulant Borderline Personality Disorder following a suicidal episode and inpatient stay. As a social worker within the mental health community, and knowing the negativity behind Borderline Personality Disorder, my world came crashing down with my diagnosis.
I began to think, “What if no one wants to work with me because I have this illness? What if my friends and family will no longer see me the same? What if no one will understand?”
I have always been an introverted, quiet person, and I didn’t see myself as exhibiting the stereotypical criteria of manipulation or explosive anger. The anger I have experienced has always been towards myself. I have a history of self-harming behavior and suicidal ideation, but I had never connected Borderline Personality Disorder to my symptoms — possibly out of the negativity I have witnessed surrounding the disease. When learning about mental illnesses in school, I wasn’t taught the different types of BPD, which added to my confusion and feelings of self-hatred and failure. Along with BPD I was also diagnosed with Complex Post Traumatic Stress Disorder (C-PTSD) and Major Depressive Disorder (MDD), and having three new diagnoses was overwhelming and hard for me to grasp. However, I felt extensive shame with my BPD diagnosis that I did not feel with the C-PTSD or MDD, and that called me to look further into the illness.
Being the natural scholar that I am, I followed my treatment with extensive research into BPD, and I discovered that Discouraged (or Quiet) BPD is the most misdiagnosed form of BPD due to the symptoms correlating with depression. Many professionals aren’t taught extensively about the subtypes of BPD, which can lead to a general lack of knowledge in the mental health field and a line of misdiagnoses in a person’s timeline, which is most likely why it took me going inpatient to be properly diagnosed. D-BPD is the most dangerous form of BPD because its sufferers don’t often reach out for help due to a feeling of inadequacy and lack of self-care, and self-harming or suicidal behaviors can often go unnoticed. I learned that intense relationships are also a factor with D-BPD, but those with the illness often sabotage their own relationships due to a belief that they don’t deserve to be loved. All of these factors hit a cord with me and they made me look at myself like I never had. I had to confront my history of intense and dysfunctional relationships as well as my isolating behavior and inconsistencies with my mood.
Broadening my knowledge made me more aware of all forms of BPD, especially understanding that the diagnosis is often connected to past trauma that the survivor couldn’t control. While BPD can come off as aggressive, it is linked to trauma and feeling defenseless, which is often overlooked. Empathy is necessary for anyone to understand what a person with BPD has gone through, especially in the mental health field. Following my experience and my research, I was relieved to know that there is a reason behind why I am the way that I am, and that there is help for all forms of BPD through Dialectical Behavior Therapy.
References
I have since been certified in Dialectical Behavior Therapy, and I am extremely passionate about helping others who have been affected by BPD and/or PTSD, or those who would like to learn more about either illness. Understanding my diagnosis not only helped me to better understand myself, it helped me to understand all affected by the disease and to realize that there is help. Survivors of BPD shouldn’t suffer due to misunderstanding and lack of knowledge, and it is my mission to ensure that BPD education and treatment is highly accessible for all. I will be exploring each form of BPD more in depth in future posts, as well as C-PTSD and PTSD.
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA: American Psychiatric Association, 2013
OPI. (2018, October 3). Understanding Self-Destructive Borderline Personality Disorder. Retrieved from https://www.optimumperformanceinstitute.com/bpd-treatment
About the Creator
Ashley Nestler, MSW
Ashley Nestler is a Bibliotherapist and a survivor of Schizoaffective Disorder, OCD, Quiet Borderline Personality, Fibromyalgia,multiple eating disorders, and C-PTSD. Ashley has dedicated her life to books and advocating for mental health.
Keep reading
More stories from Ashley Nestler, MSW and writers in Psyche and other communities.
Hidden Costs and Lasting Shame of Financial Abuse
I’ve always been responsible with my money. I have a job that pays decently, although (like many in our inflated economy) I should definitely be making more for what I do. I regularly check my credit score. I don’t eat out much, nor do I spend frivolously on non-essentials.
By Veronica Wren17 days ago in Psyche
TICK TOCK
11.59. Even though the glass had shattered, Lorna could still see that her watch ticked over. One minute until midnight. Her watch was the only thing she had that she could carry. The only thing to remember her parents by. A birthday present from last year, the year she turned seventeen.
By Elizabeth Butler4 days ago in Fiction




Comments
There are no comments for this story
Be the first to respond and start the conversation.