
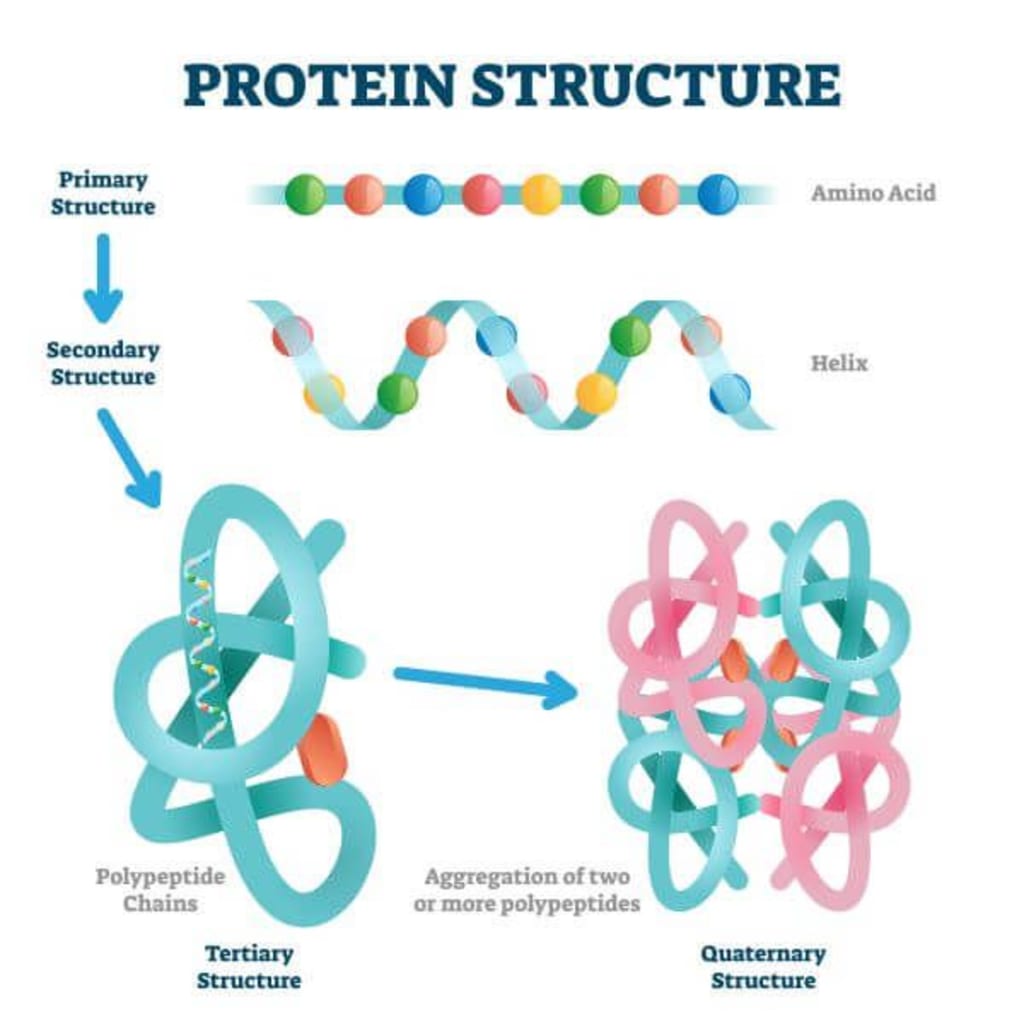
Proteins
= complex organic substances that have amino acids in their structure
Functions of proteins:
- energy role - by burning a gram of protein => 4.3 cal
- structural role
- enzymatic role
- role of hormone
- role in maintaining osmotic colloid pressure
- role in maintaining the acid-base balance
- role in defense
Proteins are:
- of animal origin
- of vegetable origin
balanced diet contains: -60% protein of vegetable origin
-40% vegetable protein
Catabolism products
= substances that are released as a result of protein metabolism and which are normally released through the kidneys
The normal protein intake is 1g / kg body weight.
All proteins are made up of amino acids and have different functions => protein specificity is given by the sequencing of amino acids in the protein structure - the sequence of amino acids in the protein structure is responsible for the specificity of each protein.
Normal value of total serum proteins - 6-8.5g%
Electrophoresis
= separation of protein fractions in the electric field; it is based on the different migration rate of proteins that depends on the number of electrical charges of the protein molecules.
o Separate the following fractions:
• albumin 45-60%
• globulins:
α1-3-7%
α2-8-12%
β- 10-14%
γ- 18-23%
a. By immunoelectrophoresis (coupling with antibodies after separation in the electric field) γ globulins are separated into the following immunoglobulins: IgA, IgM, IgD, IgE, IgG.
o Almost all proteins are synthesized in the liver except for globulins which are synthesized in the lymphoplasmacytic system.
Plasma protein systems
Renin-angiotensin-aldosterone system
- involved in homeostasis of blood pressure
- when we have an arterial hypoirrigation-> hemorrhage that leads to decreased blood levels or fluid loss => hemoconcentration- stasis occurs and renal hyperperfusion occurs- stimulates the production of renin that acts on the angiotensinogen in the liver; angiotensinogen leads to the formation of angiotensin1 which under the action of a conversion enzyme is transformed into angiotensin2 (it has 8 amino acids and is one of the most powerful vasoconstrictors in the body); angiotensin 2 increases adrenal production in the adrenal gland; Aldosterone promotes sodium reabsorption followed by water reabsorption
- activation of the renin-angiotensin-aldosterone system will result in increased sodium reabsorption followed by increased water reabsorption => increased blood volume => increased angiotensin production2
There is a system of plasma quinines - bradykinin, lysyl bradykinin, methionylisyl bradykinin.
Disorders of protein metabolism
1. Hyperproteinemia - increase in proteinemia over 8.5g%
2. Hypoproteinemia - decrease in proteinemia below 6g%.
o Both hyperproteinemias and hypoproteinemias are of two types: - apparent and real.
a. Apparent hyperproteinemia - blood serum concentration
b. Real hyperproteinemia - by intensifying the synthesis - monoclonal gamopathies - during this condition there is an anarchic (malignant) tumor proliferation of an Ig clone - a single fraction of Ig (IgM and IgG) grows
Ex: multiple myeloma, plasmacytoma
Hypoproteinemia
Causes:
deficient protein intake-in terms of quantity (uncommon) -insufficient intake: prolonged fasting, pers. with mental and neurological disorders.
In terms of quality
a. poor absorption:
- in inflammatory bowel disease
- glutemic enteropathy
- intestinal resections
- exacerbation of intestinal bacterial flora
b. synthesis deficiency - liver cirrhosis, liver cancer, acute hepatitis.
c. exaggerated losses
- renal (nephrotic syndrome - 3.5 grams of protein are lost)
- digestive (exudative enteropathy)
- plasmorrhea
- skin (burns)
Proteins are filtered glomerularly, but all are reabsorbed at the level of the proximal convoluted tube => in the final urine there are fine traces of proteins (tubular proteins, IgA).
In nephrotic syndrome, proteins appear in the final urine with low molecular weight - pure nephrotic syndrome; or high molecular weight - impure nephrotic syndrome
dysproteinaemias
= change in the concentration of serum protein fractions.
- can be: hereditary and secondary.
1. Inheritance:
are based on the lack of a protein fraction.
Example:
Analbunimenia, atransferinemia, transcobalamin deficiency (manifested by megaloblastic anemia) etc.
2. Secondary
a. Reactive dysproteinemia from acute inflammation
Alpha 1 and alpha 2 globulins increase, albumin decreases.
b. Dysproteinemia in liver disease
In chronic hepatitis and liver cirrhosis, polyclonal hyperimmunoglobulinemia occurs as a result of the chronic inflammatory process.
About the Creator
Keep reading
More stories from Nagy Alexandra and writers in Longevity and other communities.
Weight Loss Mindset: 5 Limiting Mindsets that Make Weight Loss Difficult
Have you ever attempted to lose weight? I've been there before. Even just a few months ago. For the last 30 years, I've assisted patients who wanted to improve their health. I studied how a weight loss mentality influences people and how such mindsets make weight loss challenging as a technical expert at listening to people. The good news is that we will triumph!
By Vijay Mistry6 days ago in Longevity



Comments
There are no comments for this story
Be the first to respond and start the conversation.