
What Women Should Know About Polycystic Ovary Syndrome (PCOS)
Some women, especially those of childbearing age, develop a common health condition known as Polycystic Ovary Syndrome, which is also called PCOS.

What is Polycystic Ovary Syndrome?
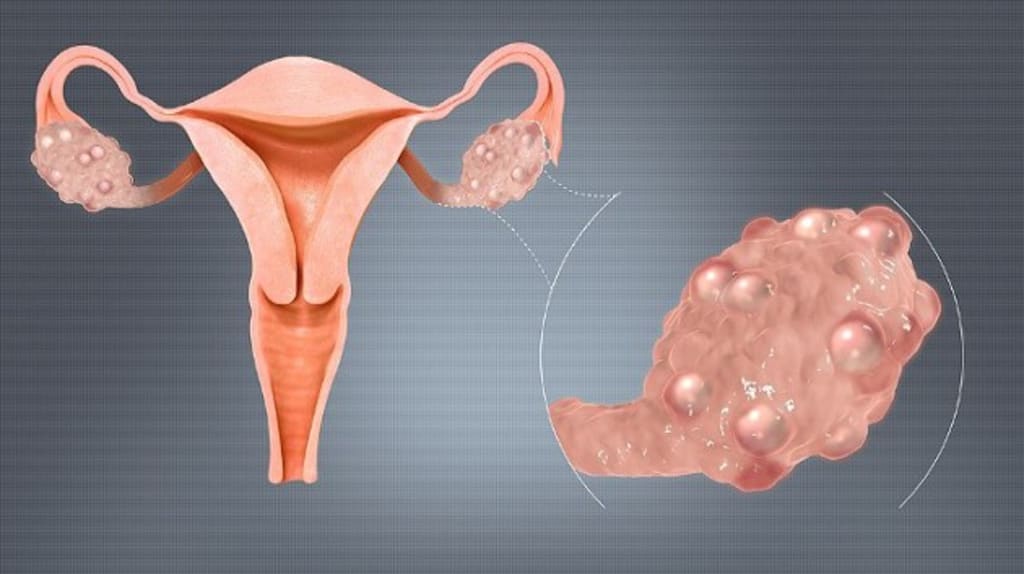
Polycystic Ovary Syndrome is caused by an imbalance of reproductive hormones, which creates problems in the ovaries. Ovaries make the egg that is released every month during a woman’s menstrual cycle. The effect of Polycystic Ovary Syndrome is that the egg may not develop as it’s supposed to or it may not be released as it should be during a woman’s ovulation process.
PCOS can cause a woman to miss her period or to have an irregular menstrual cycle. Irregular periods can cause an inability to get pregnant, known as infertility. Thus Polycystic Ovary Syndrome is one of the main reasons women become infertile. Polycystic Ovary Syndrome can also result in the development in the ovaries of small fluid sacs known as cysts. However, although Polycystic Ovary Syndrome has the word “ovary” in its name, not every woman with Polycystic Ovary Syndrome has cysts on her ovaries.
Women with Polycystic Ovary Syndrome can produce more testosterone when they have the syndrome, which means that they can build muscle easier than women without Polycystic Ovary Syndrome. Another important thing to consider is that women with Polycystic Ovary Syndrome can develop type 2 diabetes. Type 2 diabetes is nearly 3 times higher during middle age in women who have Polycystic Ovary Syndrome than in the female population in general.
PCOS can affect the fertility of a woman in different ways, with problems ovulating often being the primary cause of infertility. Even if ovulation occurs, a hormone imbalance may prevent the lining of the uterus from developing correctly to allow the implantation of a mature egg.
You should find answers to your questions about Polycystic Ovary Syndrome, as well as related topics such as In Vitro Fertilization (IVF), in the sections that follow.
While PCOS has no cure at this time, it is a condition that is treatable to reduce any adverse effects, including and especially on a woman’s ability to get pregnant and have a child.
Who gets Polycystic Ovary Syndrome?
One in 10 women of childbearing age gets Polycystic Ovary Syndrome. Women who have the syndrome develop metabolism problems and a hormonal imbalance that may affect their appearance and health overall. The syndrome is also a common cause of infertility, but that condition is treatable.
A certain percentage (between 5% and 10%) of women who are 15 to 44 years old — the years they can have children — have the syndrome. When women in their 20s and 30s have trouble getting pregnant, they go to see their doctor. That’s usually when they find out they have Polycystic Ovary Syndrome.
However, keep in mind that a woman can get the syndrome at any age after puberty, including women of all ethnicities and races. The risk is higher if you are obese or have a close female relative with the syndrome, such as an aunt, sister, or mother.
What are the symptoms of Polycystic Ovary Syndrome I should look for?
Some PCOS symptoms are:
— An irregular menstrual cycle, causing a woman to miss periods or have fewer than eight periods in a year. Or, conversely, periods may happen more often, every 21 days or more frequently. In some cases, there are some women with the syndrome who stop entirely having menstrual periods.
— Hirsutism, or having too much hair on the chin, face, or other places on the body where men usually have hair. Studies show that 70% of women with the syndrome have hirsutism.
— Acne on the upper back, face, and chest.face, chest
— Hair loss on the scalp or thinning hair, also known as male-pattern baldness
— Difficulty losing weight or weight gain
— Darkening of the skin, particularly underneath breasts, along neck creases, and in the groin area
— Skin tags, which are small flaps of excess skin in the neck area or armpits
What causes Polycystic Ovary Syndrome?
What causes PCOS isn’t known. However, most experts believe that genetics and several other factors play a role:
— High levels of androgens, which are sometimes called “male hormones.” Every woman produces small amounts of androgens, but having the syndrome can significantly increase the amount, causing a woman to have more than normal. This results in the development of male traits, such as male-pattern baldness.
If a woman has a higher than normal androgen level it can prevent her from ovulating (releasing an egg) during her menstrual cycles. This can cause acne and extra hair growth, which are two signs of the syndrome.
— High levels of insulin, the hormone that controls how the food you eat is converted into energy. A woman who suffers from insulin resistance means that her body’s cells do not respond in the usual way to insulin. Thus, her insulin blood levels become higher than is normal.
A woman is more susceptible to the syndrome if she is obese or overweight, doesn’t get enough physical exercise, has unhealthy eating habits, or has a history of diabetes in her family (usually type 2). Over time resistance to insulin can lead to type 2 diabetes.
If I have Polycystic Ovary Syndrome can I still get pregnant?
Yes, a woman with PCOS can still get pregnant. The syndrome can make a woman infertile, which is a hormonal imbalance that interferes with the process of ovaries growing and releasing eggs (ovulation). You can’t get pregnant if you don’t ovulate. The good news is that infertility is very treatable.
What other health problems is Polycystic Ovary Syndrome linked to?
Studies have shown links between the syndrome and some other health problems, including:
— Diabetes. Before the age of 40, more than half of the women with Polycystic Ovary Syndrome will have prediabetes (glucose intolerance) or diabetes.
— High blood pressure. When compared with women who are the same age and without PCOS, women who have the syndrome have a greater risk of having high blood pressure, which is a significant cause of stroke and heart disease.
— Unhealthy cholesterol. Women with the syndrome often have low levels of HDL (good) cholesterol and higher levels of LDL (bad) cholesterol. If you have high cholesterol, it raises your risk of heart disease and stroke.
— Sleep apnea, which is when your breathing is repeatedly or momentarily interrupted or stopped during sleep. Because many women with the syndrome are overweight or obese, they may develop sleep apnea, which increases their risk of heart disease as well as diabetes.
— Anxiety and depression. It’s common among women with Polycystic Ovary Syndrome to have anxiety and depression.
— Endometrial cancer. Women with the syndrome often have problems with diabetes, insulin resistance, obesity, and ovulation. These factors increase the risk of developing cancer in the lining of the uterus or womb, the endometrium.
Researchers are not sure about whether PCOS causes some of the above-listed problems, or if other conditions cause the syndrome and other health problems, or if these problems cause Polycystic Ovary Syndrome.
When I reach menopause will my Polycystic Ovary Syndrome symptoms go away?
The answer is yes and no. Although PCOS affects many systems in the body, the menstrual cycles of many women with the syndrome become more regular, the closer they get to menopause. However, they may continue to have symptoms of the syndrome because their hormonal imbalance does not change with age.
Also, the risks of syndrome-associated health problems, such as heart attack, stroke, and diabetes, increase with age. These particular risks may be higher in women with the syndrome than those without it.
How do I diagnose Polycystic Ovary Syndrome?
There isn’t a single test for diagnosing PCOS, so your doctor may discuss your medical history with you and do a physical exam along with different tests. This process helps diagnose whether you have Polycystic Ovary Syndrome and can rule out other causes of your symptoms. To make the diagnosis, the doctor will do the following:
— Pelvic exam. A pelvic exam may be performed to check for any indications of additional male hormones (such as an enlarged clitoris) and check to see if your ovaries are enlarged or swollen.
— Pelvic ultrasound (sonogram), which uses sound waves to examine your ovaries, especially the lining of the uterus or womb for cysts, to see if you have the condition known as the endometrium.
— Physical exam, during which our doctor will measure your waist size, body mass index (BMI), and blood pressure. The doctor will also look at your skin for extra hair on your back, chest, and face, and acne and skin discoloration. Your doctor may check for signs of other health conditions (such as an enlarged thyroid gland) and any hair loss.
— Blood tests to check your androgen hormone levels, sometimes referred to as “male hormones.” Also, your doctor will check for other hormones related to other common health problems, such as thyroid disease, which can be mistaken for the syndrome. Finally, your doctor may also test you for diabetes and your cholesterol levels.
Once other conditions are ruled out, if you have two of the following conditions you may be diagnosed with Polycystic Ovary Syndrome:
— Irregular periods that don’t come often enough, come too often, or don’t come at all
— Indications of high levels of androgens:
— Extra hair growth on your body, chin, and face (hirsutism)
— Acne
— Scalp hair that’s thinning
— Blood levels of androgens that are higher than normal
— One or both ovaries with multiple cysts (Note: Despite its name, not all women with the syndrome have ovary cysts.)
Women with Polycystic Ovary Syndrome have more testosterone and can build muscle easier than women without the syndrome. Also, type 2 diabetes in women at middle age who have the syndrome is nearly seven times higher than the rate of the female population overall.)
How do I treat Polycystic Ovary Syndrome?
Even though there currently is no cure for PCOS, you can manage its symptoms. Based on what your symptoms are, your risk of long-term health problems such as diabetes and heart disease, and your plans for having children, you and your doctor can develop a treatment plan that encompasses a combination of treatments, including:
— Using medicines
— By steps you can take at home that will help relieve your symptoms, such as:
— Losing weight, by practicing healthy eating habits (e.g., by eating a low-carb, high-fat diet), and by doing regular physical activity, can help relieve symptoms related to the syndrome. If you lose weight, it may improve the way your body uses insulin, help your hormones reach normal levels, and also help to lower your blood glucose levels. Even a bodyweight of 10% (for example, if a 150-pound woman loses 15 pounds) can help improve your menstrual cycle by making it more regular and increase your chances of getting pregnant. Learn more about healthy weight.
— Removing hair using procedures such as laser hair removal or electrolysis; a doctor must perform these methods and health coverage may not cover them. Laser hair removal, electrolysis, or facial hair removal creams are methods you can try to remove excess hair. If you want to try to do it yourself with hair removal creams and products, you can easily find them at drugstores.
— Slowing hair growth by using prescription skin treatment (eflornithine HCl cream), which can help slow down the rate of growth of new hair in unwanted places.
What types of medicines should I use to treat Polycystic Ovary Syndrome?
You can treat PCOS and its symptoms with various medicines, including:
— Anti-androgen medications, which block the effect of androgens and can help reduce acne, body and facial hair growth, and scalp hair loss. It’s important to note this type of medicine is not approved by the Food and Drug Administration (FDA) to treat symptoms of Polycystic Ovary Syndrome. Also, you must exercise caution because anti-androgen medicines can also cause problems during pregnancy.
— Metformin, which may help some women with symptoms of the syndrome, is often used to treat type 2 diabetes. However, the FDA has not yet approved Metformin to treat the symptoms of Polycystic Ovary Syndrome. Metformin works by improving the ability to lower your blood sugar as well as lower both androgen and insulin levels. Metformin may help restart ovulation after a few months of use. However, it usually has little effect on excess hair on the body or face or acne. According to research conducted recently, there may be other positive benefits from using Metformin, including improving cholesterol and lowering body mass.
— Hormonal birth control, including an intrauterine hormone device (IUD), vaginal ring, patch, shot, and the pill. If a woman doesn’t want to get pregnant, the use of hormonal birth control can result in:
— A more regular menstrual cycle
— Lower risk of endometrial cancer
— Improve acne condition and reduce excess hair on the body and face (Be sure to ask your doctor about birth control that uses both progesterone and estrogen.
How does Polycystic Ovary Syndrome affect me if I become pregnant?
During your pregnancy, PCOS may cause problems for both you and your baby because women with the syndrome have higher rates of:
— Cesarean section (C-section)
— Preeclampsia
— Gestational diabetes
— Miscarriage
Your baby may spend more time in a neonatal intensive care unit (NICU) and might also have a higher risk of being heavy (macrosomia).
What can I do to prevent problems from Polycystic Ovary Syndrome during my pregnancy?
To lower your risk of problems from PCOS during pregnancy, you can:
— Make sure you are at a healthy weight before you get pregnant.
— Reach healthy blood sugar levels before getting pregnant by a combination of medicines such as Metformin, weight loss, healthy eating habits, and regular physical activity.
— Take folic acid but be sure to find out how much folic acid you need by talking to your doctor.
What are my treatment options for Polycystic Ovary Syndrome if I want to get pregnant?
Several options available to you to increase your chances of getting pregnant if you have PCOS:
— Losing weight. If you are obese or overweight, losing weight through exercising regularly and by healthy eating improves your fertility by making your menstrual cycle more regular.
— Medicine. After you and your partner have ruled out other causes of infertility, your doctor might prescribe a medicine such as clomiphene (Clomid) to help you ovulate.
— Surgery. Although surgery is an option, usually you would choose to go that route only if other options haven’t worked. In other words, consider surgery to be your last resort.
— In Vitro Fertilization (IVF). In Vitro Fertilization is used to help a woman get pregnant. If medicines alone don’t work, In Vitro Fertilization may be a good option for you. In Vitro Fertilization uses a combination of surgical procedures and drugs to help with the fertilization process.
The way In Vitro Fertilization works is that you use your partner’s sperm to fertilize your egg by placing the sperm in your uterus so that it is implanted there and can develop. The procedure for fertilizing an egg is performed using a dish in a laboratory and usually takes from four to six weeks.
Compared to medicine alone, In Vitro Fertilization results in higher pregnancy rates and allows you better control over the risk of you having twins and triplets because your doctor transfers just a single fertilized egg into your uterus. Typically, most women see success rates with In Vitro Fertilization of 20–35% per cycle.
However, the chances of you getting pregnant decreases with each successive In Vitro Fertilization round, while the cost increases. If you have three full cycles of In Vitro Fertilization, the cumulative effect is that your chances of a successful pregnancy increase to 45–53%. The bottom line is that In Vitro Fertilization is generally successful for women of all ages, with the odds of a live birth being between 34 and 42 percent over three cycles. The success rate is particularly good for women under age 35 and those using donor eggs.
What are the chances of me getting pregnant if I use In Vitro Fertilization?
It’s typical for most women to achieve success rates of 20–35% per cycle when using In Vitro Fertilization. While it would be great if you got pregnant after your first In Vitro Fertilization cycle, there is no guarantee of that so you may require additional cycles. However, the chances of your getting pregnant decrease with each successive round, while the cost increases. The cumulative effect of three full cycles of the procedure increases the odds of a successful pregnancy to 45–53%.
A vast majority of women with Polycystic Ovarian Syndrome who haven’t become pregnant with other treatments can get pregnant and have a baby using In Vitro Fertilization. This situation is especially true if they use a high-quality clinic and are under the age of 40.
Signs of a successful In Vitro Fertilization include:
— Light spotting
— Cramping
— Fatigue
— Nausea
— Sensitive breasts
Remember that all of the above symptoms can and do occur even if you’re not pregnant. You may have absolutely no pregnancy symptoms and still, be pregnant.
What helps my fertility if I have Polycystic Ovary Syndrome?
— Fertility treatments for PCOS
— Fertility medications. Fertility drugs may help symptoms of Polycystic Ovary Syndrome in an attempt to assist with ovulation temporarily.
— Metformin. Fertility drugs for PCOS often are taken in combination with Metformin.
— Ovarian drilling
— Natural Polycystic Ovary Syndrome fertility aids
— IVF
Conclusion
This article discussed in detail various vital aspects of Polycystic Ovary Syndrome, as well as covering related topics such as In Vitro Fertilization. While PCOS has no cure at this time, it is a condition that is treatable to reduce any adverse effects, including and especially on a woman’s ability to get pregnant and have a child.
So if you or any other woman you know who is of childbearing age, has or may have Polycystic Ovary Syndrome, please do yourself a big favor health-wise and stay as well-informed as possible about these extremely important issues.
Note: The information in this article should not be considered as professional medical advice, diagnosis, or treatment. It is for informational purposes only and represents the author’s opinions alone based on research conducted.
Reference sources:
Healthy Smarts MD, The Endocrine Society, The American Society for Reproductive Medicine, Office of Women’s Health/US Dept. of Health and Human Services, The American Association of Clinical Endocrinologists, The American Diabetes Association, The American College of Obstetrics and Gynecology.
__________________
Thanks for reading. Copyright © Terry Mansfield. All Rights Reserved.
About the Creator
Terry Mansfield
Trying to be the best writer I can be. Specialist in eclecticism.
Keep reading
More stories from Terry Mansfield and writers in Viva and other communities.
Thank You Female Product Companies For Normalizing Human
I was born in 1990. In May, smack dab early mid-year. I am quite LITERALLY the definition of a '90's' kid. I don't remember a lot of commercials from when I was younger, but I do know that growing up women in media were photoshopped, sculpted, and molded to be Barbie perfect.
By Hope Martin16 days ago in Viva
Navigating the Ocean of Confidence: Maya's Journey Towards True Self-Belief
Once upon a time, in a bustling city nestled between towering skyscrapers and bustling streets, there lived a young woman named Maya. Maya was like any other person in the city, going about her day, working hard, and trying to find her place in the world. But deep down, Maya struggled with something that many people face at some point in their lives: self-confidence.
By Wishorizon762 days ago in Viva
In The Blink of Her Eye
Time itself bent and morphed, allowing Shannon the precious seconds needed to see and adjust to the disaster unfolding in front of her. Each frame showed minute details she would have missed had the clock not slowed down until she heard every click of the hands as they swept toward the end of everything. If only she was being melodramatic...
By Lisa VanGalen2 days ago in Fiction




Comments
There are no comments for this story
Be the first to respond and start the conversation.