


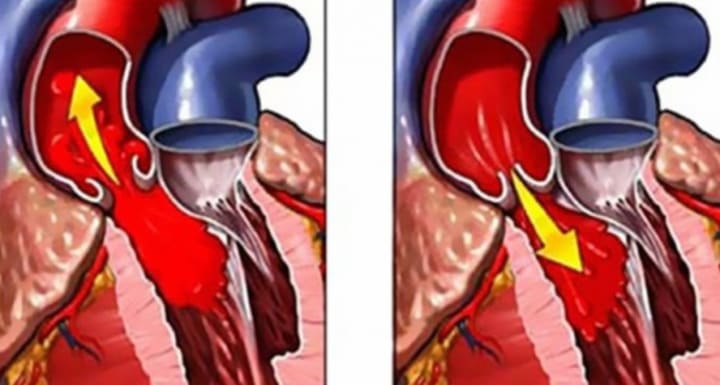
Aortic insufficiency is an incomplete closure of the aortic valve flaps during diastole, leading to a reverse flow of blood from the aorta to the left ventricle. Aortic insufficiency is accompanied by dizziness, fainting, chest pain, shortness of breath, frequent and irregular heartbeat. To diagnose aortic insufficiency, chest X-ray, aortography, EchoCG, ECG, MRI and CT of the heart, cardiac catheterization, etc. are performed. Treatment of chronic aortic insufficiency is carried out conservatively (diuretics, ACE inhibitors, calcium channel blockers, etc.); in severe symptomatic course, plastic surgery or prosthetics of the aortic valve is indicated.
General information
Aortic insufficiency (aortic valve insufficiency) is a valvular defect in which, during diastole, the semilunar flaps of the aortic valve do not completely close, resulting in diastolic regurgitation of blood from the aorta back into the left ventricle. Among all heart defects, isolated aortic insufficiency accounts for about 4% of cases in cardiac surgery; in 10% of cases, aortic valve insufficiency is combined with other valvular lesions. In the vast majority of patients (55-60%), a combination of aortic valve insufficiency and aortic stenosis is detected. Aortic insufficiency is 3-5 times more common in males.
Reasons
Aortic insufficiency is a polyethological defect, the origin of which may be due to a number of congenital or acquired factors. Congenital aortic insufficiency develops in the presence of a one–, two- or four-leaf aortic valve instead of a tricuspid one. In this case, there is usually an incomplete closure or prolapse of the aortic valve. The causes of aortic valve defect can be hereditary connective tissue diseases:
- aortoannular ectasia;
- Marfan syndrome;
- Ehlers-Danlos syndrome;
- cystic fibrosis;
- congenital osteoporosis;
- Erdheim's disease, etc.
The main causes of acquired organic aortic insufficiency are:
- rheumatism (up to 80% of all cases);
- septic endocarditis;
- atherosclerosis;
- syphilis;
- rheumatoid arthritis;
- systemic lupus erythematosus;
- Takayasu's disease;
- traumatic valve injuries, etc.
Rheumatic lesion leads to thickening, deformation and wrinkling of the aortic valve flaps, as a result of which their full closure does not occur during diastole. Rheumatic etiology usually underlies the combination of aortic insufficiency with mitral malformation. Infectious endocarditis is accompanied by deformation, erosion or perforation of the valves, causing a defect of the aortic valve.
The occurrence of relative aortic insufficiency is possible due to the expansion of the fibrous ring of the valve or the aortic lumen in arterial hypertension, Valsalva sinus aneurysm, delaminating aortic aneurysm, ankylosing rheumatoid spondylitis (Bekhterev's disease), and other pathologies. In these conditions, separation (divergence) of the aortic valve flaps during diastole may also be observed.
Pathogenesis
Hemodynamic disorders in aortic insufficiency are determined by the volume of diastolic regurgitation of blood through a valve defect from the aorta back to the left ventricle (LV). At the same time, the volume of blood returning to the LV can reach more than half of the cardiac output.
Thus, in aortic insufficiency, the left ventricle during diastole is filled both as a result of blood flow from the left atrium and as a result of aortic reflux, which is accompanied by an increase in diastolic volume and pressure in the LV cavity. The volume of regurgitation can reach up to 75% of the stroke volume, and the final diastolic volume of the left ventricle can increase to 440 ml (with a norm of 60 to 130 ml).
The expansion of the cavity of the left ventricle contributes to the stretching of muscle fibers. To expel the increased volume of blood, the force of ventricular contraction increases, which, with a satisfactory condition of the myocardium, leads to an increase in systolic output and compensation for altered intracardiac hemodynamics. However, prolonged operation of the left ventricle in hyperfunction mode is invariably accompanied by hypertrophy, and then cardiomyocyte dystrophy: a short period of LV tonogenic dilatation with an increase in blood outflow is replaced by a period of myogenic dilatation with an increase in blood flow. As a result, mitralisation of the defect is formed - relative insufficiency of the mitral valve due to LV dilation, impaired function of papillary muscles and expansion of the fibrous ring of the mitral valve.
In conditions of compensation for aortic insufficiency, the function of the left atrium remains undisturbed. With the development of decompensation, there is an increase in diastolic pressure in the left atrium, which leads to its hyperfunction, and then hypertrophy and dilation. Stagnation of blood in the system of vessels of the small circulatory circle is accompanied by an increase in pressure in the pulmonary artery, followed by hyperfunction and hypertrophy of the myocardium of the right ventricle. This explains the development of right ventricular failure in aortic malformation.
Classification
To assess the severity of hemodynamic disorders and compensatory capabilities of the body, a clinical classification is used that identifies 5 stages of aortic insufficiency:
I - stage of complete compensation. Initial (auscultative) signs of aortic insufficiency in the absence of subjective complaints.
II - stage of latent heart failure. A moderate decrease in exercise tolerance is characteristic. According to the ECG data, signs of hypertrophy and volumetric overload of the left ventricle are revealed.
III - stage of subcompensation of aortic insufficiency. Typical anginal pain, forced restriction of physical activity. ECG and radiographs show hypertrophy of the left ventricle, signs of secondary coronary insufficiency.
IV - stage of decompensation of aortic insufficiency. Severe shortness of breath and attacks of cardiac asthma occur at the slightest strain, an increase in the liver is determined.
V - terminal stage of aortic insufficiency. It is characterized by progressive total heart failure, deep dystrophic processes in all vital organs.
Symptoms of aortic insufficiency
Patients with aortic valve insufficiency in the compensation stage do not notice subjective symptoms. The latent course of the defect can be long – sometimes for several years. The exception is acute aortic insufficiency caused by a delaminating aortic aneurysm, infectious endocarditis and other causes.
Symptoms usually manifest with sensations of pulsation in the vessels of the head and neck, increased cardiac tremors, which is associated with high pulse pressure and increased cardiac output. Sinus tachycardia, characteristic of aortic insufficiency, is subjectively perceived by patients as a rapid heartbeat.
With a pronounced valve defect and a large volume of regurgitation, brain symptoms are noted: dizziness, headaches, tinnitus, visual disturbances, short-term fainting states (especially with a rapid change of the horizontal position of the body to the vertical).
In the future, angina pectoris, arrhythmia (extrasystole), shortness of breath, increased sweating are added. In the early stages of aortic insufficiency, these sensations worry mainly during exercise, and later occur at rest. The addition of right ventricular insufficiency manifests itself as swelling on the legs, heaviness and pain in the right hypochondrium.
Complications
Acute aortic insufficiency occurs according to the type of pulmonary edema combined with arterial hypotension. It is associated with a sudden volumetric overload of the left ventricle, an increase in the final diastolic pressure in the LV and a decrease in shock output. In the absence of special cardiac surgery, mortality in this condition is extremely high.

Diagnostics
Physical data in aortic insufficiency are characterized by a number of typical signs. On external examination, attention is drawn to the pallor of the skin, in the later stages – acrocyanosis. Sometimes external signs of increased pulsation of the arteries are detected – "carotid dance" (visible pulsation on the carotid arteries), Musset symptom (rhythmic nodding of the head to the beat of the pulse), Landolfi symptom (pulsation of the pupils), "Quincke capillary pulse" (pulsation of the vessels of the nail bed), Muller symptom (pulsation of the tongue and soft palate).
A typical visual definition of the apical shock and its displacement in the VI-VII intercostal space; pulsation of the aorta is palpated behind the xiphoid process. Auscultative signs of aortic insufficiency are characterized by diastolic noise on the aorta, weakening of the I and II heart tones, "accompanying" functional systolic noise on the aorta, vascular phenomena (double Traube tone, double Durosier noise). Instrumental diagnosis of aortic insufficiency is based on the results:
- ECG. Electrocardiography reveals signs of hypertrophy of the left ventricle, with mitralisation of the defect - data for hypertrophy of the left atrium.
- Phonocardiography. With the help of phonocardiography, altered and pathological cardiac noises are determined.
- X-ray studies. Chest X-rays reveal the expansion of the left ventricle and the shadow of the aorta, the displacement of the apex of the heart to the left and down, signs of venous stagnation of blood in the lungs. With ascending aortography, the regurgitation of blood flow through the aortic valve into the left ventricle is visualized. Additional methods are MRI, MSCT.
- EchoCG. Echocardiographic examination reveals a number of characteristic symptoms of aortic insufficiency - an increase in the size of the left ventricle, an anatomical defect and functional failure of the aortic valve.
- Cardiac catheterization. Probing of the heart cavities in patients with aortic insufficiency is necessary to determine the magnitude of cardiac output, the final diastolic volume in the LV and the volume of regurgitation, as well as other necessary parameters.
Treatment of aortic insufficiency
A mild degree of aortic insufficiency with an asymptomatic course does not require treatment. It is recommended to limit physical activity, annual examination by a cardiologist with EchoCG. In asymptomatic moderate aortic insufficiency, diuretics, calcium channel blockers, ACE inhibitors, angiotensin receptor blockers are prescribed. In order to prevent infection during dental and surgical manipulations, antibiotics are prescribed.
Surgical treatment - plastic surgery / prosthetics of the aortic valve is indicated for severe symptomatic aortic insufficiency. In the case of acute aortic insufficiency due to delamination of an aneurysm or aortic injury, prosthetics of the aortic valve and the ascending aorta are performed. Signs of inoperable are an increase in LV diastolic volume to 300 ml; ejection fraction of 50%, final diastolic pressure of the order of 40 mm Hg.
Prognosis and prevention
The prognosis of aortic insufficiency is largely determined by the etiology of the defect and the volume of regurgitation. With severe aortic insufficiency without decompensation, the average life expectancy of patients from the moment of diagnosis is 5-10 years. In the decompensated stage with the phenomena of coronary and heart failure, drug therapy is ineffective, and patients die within 2 years. Timely cardiac surgery significantly improves the prognosis of aortic insufficiency.
Prevention of the development of aortic insufficiency consists in the prevention of rheumatic diseases, syphilis, atherosclerosis, their timely detection and full-fledged treatment; medical examination of patients at risk for the development of aortic malformation.
About the Creator
Artur Kh.
Writer, doctor and businessman. I blog about self-development, personal growth, health and new ways of making money.
Say Goodbye to Hangnails: Expert Tips and Tricks
A terrible hangnail can ruin your day. Inflammation, throbbing, delicate tiny skin tears can cause aches. "There are a lot of sensitive nerve endings in the fingers, so the skin is exceptionally delicate," said Dr. Amanda Zubek, an assistant professor of dermatology at the Yale School of Medication.
By shanmuga priyaa day ago in Blush
A New Beginning
Tony couldn’t sit still, crossing and uncrossing his legs, trying to calm his trembling hands as Clara stood at the office window deep in thought. The airline ticket in his shirt pocket moved to the beat of his heart¬– each beat bringing back the nightmare causing memories of the words he’d spoken over ten years ago. Thanks to Clara he’d finally gained the courage to buy that ticket.
By Gerald Holmes4 days ago in Fiction



Comments
There are no comments for this story
Be the first to respond and start the conversation.