
Uncover Unconscious Bias in the Medical Field
Discussing the impacts of human bias in healthcare


“Unconscious bias.” Many of us have heard of this term before, and in essence, all “unconscious bias” refers to are the biases that an individual holds that they are not aware of. Most importantly, each and every human being holds bias of some kind, meaning we are never alone in our journeys to combat unconscious bias. Of course, the universality of unconscious bias makes it no less acceptable, and it is imperative we take action to eliminate unconscious bias from all fields of life, such as the healthcare system.
Although the idea of bias in the medical system may be difficult to grasp since healthcare providers are legally prohibited from discriminating against their patients, we must remember that unconscious bias is exactly that—unconscious. For example, a doctor might outwardly support the queer community, yet assume that their woman patient who is sexually active has a male partner. In other words, the disparities that arise for marginalized groups in healthcare treatment are often unintentional, and although the provided example is a comparatively minor one, that makes these biases no less dangerous. Let’s take a look at three categories:
1. Racial and ethnic disparities
Through reviews of several hundred empirical studies, the Institute of Medicine (IOM) determined that Black Americans are particularly vulnerable to racialized healthcare disparities. Compared to white Americans, they are less likely to receive certain necessary surgeries (organ transplants, knee and hip replacements, cardiac surgeries, etc.) and are more likely to undergo certain unnecessary, or rather, preventable surgeries (diabetic amputations, castration for prostate cancer, etc.). A study by the National Hospital Ambulatory Medical Care Survey found that people of color—especially Black Americans—are less likely to be prescribed pain medications, such as opioids, for the same diseases and injuries as white people. The Journal of Internal Medicine also reported that Black patients are more likely to be labelled as “less cooperative” than white patients. This research is supported by the IOM’s findings that patients of color may be more likely to convey mistrust towards their medical providers or refuse treatment because of discriminatory interactions rooted in unconscious bias that they had with medical practitioners in the past.
Despite the severity of the above information, perhaps this is the most damning statistic of all: as determined by the IOM, the overall Black mortality rate is 60% higher than that of whites. Such a discrepancy is terrifying and speaks to the imminent need to combat unconscious bias in the medical field. Simply put, there is no question that racial and ethnic disparities in healthcare exist, and moreover that they can be deadly. Worst of all, they are not the only discriminatory discrepancies.
2. LGBTQ+ disparities
An analysis of queer populations in the National Healthcare Quality and Disparities Report as well as several other studies has revealed the prevalence of anti-queer discrimination in healthcare. About 30% of LGBTQ+ individuals have delayed care—both imminent and preventative—because of disrespect and discrimination from their providers. One in five transgender individuals have been outright refused care by doctors or other medical practitioners because of their gender, with trans people of color being more likely than white trans people to experience this refusal. A 2010 study found that a third of lesbian women avoid medical care, such as delaying necessary appointments like Pap screenings, because they fear anti-gay discrimination. Some research suggests that unconscious anti-queer bias can run so deep as to negatively impact the healthcare of children who have gay parents. Overall, LGBTQ+ communities also have less access to insurance and healthcare than cisgender, heterosexual populations. As a result of this restricted access, compounded by anti-queer discrimination, they find themselves at higher risk of certain cancers, diseases, and more. Like racial and ethnic disparities, there is no question that queer disparities in healthcare exist because of unconscious bias and that the need to take action against them is imminent.
3. Weight-based disparities
Few people deny that obesity can be a physiological health risk. However, we must also acknowledge that being obese can have dire consequences on a person’s mental health because of the discrimination (and the stress of this discrimination) that comes with being overweight. For example, stereotypes held against overweight individuals by medical providers, nurses, and the general public include but are not limited to: lazy, lacking in self-control, unsuccessful, unintelligent, and dishonest. Obesity gets written off as the fault of the overweight individual, i.e. that they are too lazy to exercise and eat healthy, when in reality the causes of weight gain are far more complicated. For example, obesity can be caused by other health conditions. It can also result from poverty (e.g. poorer people are often unable to afford healthier foods—as items like fresh fruits and vegetables tend to be more expensive—or they may live in food deserts, where these healthy items are outright unavailable to them). Simply put, a person’s weight is almost never an exclusive result of how much they exercise or eat.
Despite the inherent nuance that is therefore required to discuss obesity, the statistics of weight-based disparities in the medical field present a dismal reality. According to various studies headed by Cambridge and the University of Washington, weight-based discrimination in the United States has increased by 66% in recent years; 53% of overweight women report rude or inappropriate comments from their healthcare providers; and overall, obese patients report regular disrespect from their medical practitioners, causing them to be more likely to avoid routine care (e.g. cancer screenings). The Rudd Center found that 31% of nurses did not want to attend to overweight patients, and 24% of nurses outright admitted that overweight patients “repulsed them.” In other words, we don’t have to go far to find stories about overweight individuals who have their pain dismissed by doctors who choose to attribute any problems their obese patients present as being an exclusive result of their weight instead of conducting appropriate examinations—unconscious bias at work. Similarly, if an obese patient is struggling to lose weight, unconscious bias can lead doctors to blame this struggle on the patients’ supposed laziness or insist that the patients simply aren’t trying hard enough rather than investigating what other factors might be at play.
So, what can we do? And why does this matter to the corporate workplace?
Fortunately, there are numerous steps that can be taken to address racial, ethnic, queer, weight-based, and numerous other disparities in the medical field. Some steps are a matter of practicality, such as providing armless chairs and larger examinations gowns to better accommodate obese people in the medical locale, but these solutions must also be accompanied by more rigorous institutional change. Best of all, many of these institutional changes to combat unconscious healthcare discrimination are also applicable to other organized workplaces, including those of business and the corporate world.
The first step, as always, is education. Medical providers must be made aware that unconscious bias exists in the medical field and that healthcare disparities occur because of unconscious bias, often despite practitioners’ good intentions. Following this introductory step, medical providers should then be informed of their own unconscious biases, such as by taking Harvard’s Implicit Association Test (IAT), which has tests that examine bias in race, sexuality, disability, weight, religion, and more. Similarly, cross-cultural education should be made available to medical practitioners, as knowing more about different cultures will help practitioners develop a more diverse, accessible approach to medicine for all their patients. The application of such education to the business world is self-evident: the more educated we are about unconscious bias in our workplaces, the more we can do to address and even prevent it, and the better we can embrace our diverse employees and clients.
Beyond education, communication is also critical to combating unconscious bias in the medical field. First and foremost, researchers emphasize that trust must be established between the patient and the provider, such as using the Berlin and Fowkes LEARN model:
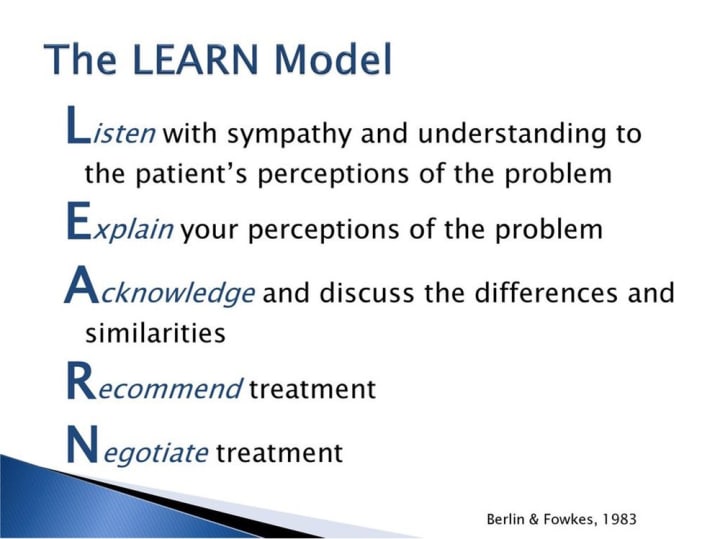
This model emphasizes the need for active and empathetic listening by the practitioner. For example, medical providers should ask patients open-ended questions and neither interrupt nor directly contradict their patient’s experiences while a patient speaks. Practitioners should also ask if their patients have any specific concerns. Moreover, medical providers must keep in mind their patients’ access to healthcare, e.g. if the patient has to take time off or arrange specific transportation to come to the doctor. In a similar vein, this type of empathetic communication is also critical to the corporate workplace, as it can help ensure diverse employees feel included and heard in their efforts toward the organization as a whole.
Speaking of the overall organization, education and communication must be accompanied by policy changes to address disparities in the medical field, such as revising regulations to acknowledge how healthcare plans often become disrupted along socioeconomic lines. These types of policy change should also be applied to the medical workplace itself. One way to determine the changes needed is to get a feel for the organizational culture of the respective medical location (hospital, doctor’s office, etc.). Organizational culture can be thought of as the unconscious biases of a collective group that unwittingly maintain a biased status quo. Conducting anonymous surveys of current and former medical employees to find out what issues they presently face as well as the issues that made people leave can provide clarification about what realms of bias need to be addressed first. The application of this strategy to the corporate workplace is therefore straightforward, as non-medical organizations, too, should get a feel for the unconscious biases within their organizational culture through items like surveys in order to better address and even eliminate these biases.
Unconscious bias in the medical field is an active threat to marginalized populations, as access to appropriate healthcare can be a life or death situation. Although this grave reality makes the task of combating these health disparities all the more intimidating, we cannot allow ourselves to back down. If making the world a better, safer place can be accomplished through strategies as straightforward as education, communication, and policy changes, then I say there’s no reason we cannot begin today.
Much to think about.
____________________________________________________
Dima Ghawi is the founder of a global talent development company with a primary mission for advancing individuals in leadership. Through keynote speeches, training programs and executive coaching, Dima has empowered thousands of professionals across the globe to expand their leadership potential. In addition, she provides guidance to business executives to develop diversity, equity, and inclusion strategies and to implement a multi-year plan for advancing quality leaders from within the organization.
Reach her at DimaGhawi.com and BreakingVases.com.
About the Creator
Dima Ghawi
Dima is an award-winning author and a three-time TEDx Speaker. Through keynote speeches, workshops, training programs, and executive coaching, she has honed a keen expertise in developing leaders to meet the demands of the global workforce.
Keep reading
More stories from Dima Ghawi and writers in Journal and other communities.
Fostering Inclusive Dialogue
The ever increasing recognition of the importance of diversity and inclusion (D&I) in the workplace comes with an expectation that we as individuals should know how to participate in and encourage inclusive conversations. ‘But that’s overwhelming!’ some of us might fret. ‘I want to get this right, but where should I start?’ Fear not—terrifying as this communication may seem, fostering inclusive dialogue is a task any of us can accomplish, whether we’re experts in D&I or just dipping our toes in the water for the first time.
By Dima Ghawiabout a year ago in Journal
25 Best Sites to Sell Feet Pics in 2024
Feet pics selling is a lucrative business opportunity for the GenZs and Millennials, but it is not only about snapping photos of feet. The business demands many more aspects for selling feet pics and making a profit out of it, and understanding where to sell them safely, is the most crucial aspect.
By Bindu Sharma6 days ago in Journal
Standing Still
There are very few moments in life where time truly stands still. When your breath is taken from your chest and your body hangs weightless in that moment. Just long enough for it to stay with you from that day onwards. Deep in the red sands of the Australian Outback, I found that moment and clung to it forever.
By Kevin McLaughlin4 days ago in Wander




Comments
There are no comments for this story
Be the first to respond and start the conversation.